Here is a sample that showcases why we are one of the world’s leading academic writing firms. This assignment was created by one of our expert academic writers and demonstrated the highest academic quality. Place your order today to achieve academic greatness. Read a guide about how to write a literature review.
Tuberculosis (TB) was declared a global health emergency by the World Health Organization (WHO) in 1993. Despite this, it remains a significant cause of mortality and morbidity throughout the world. Tomas et al. (2013) find that tuberculosis has been gradually declining since the 1990s and 2000s, with an estimated nine million incidences of tuberculosis in 2010.
TB is caused by mycobacterium tuberculosis which is an air-borne disease and transmitted when an individual with the active form of the disease sneezes, coughs, spits, or speaks (Bender, Andrews, & Peter, 2010; Bodenmann et al., 2009; Kan, Kalin, & Bruchfeld, 2013; Nuzzo, Golub, Chaulk, & Shah, 2013).
It is estimated that one-third of the global population is infected with tuberculosis, but not all infected people can develop it. The disease can remain latent, asymptomatic, and non-infectious for many years (van der Werf & Zellweger, 2016). However, in about 10% of cases, the infection can reactivate at any time (Werf & Kramarz, 2016a).
The reemergence of tuberculosis in low-prevalence industrialized countries in the West and Australia has become a public health challenge. A part of the disease’s reemergence is attributed to multiple antibiotic resistance and its interaction with AIDS/HIV (Tomás et al., 2013). According to Panchal et al. (2013),
TB is strongly connected with poverty; in developed and less developed countries, 95% of the deaths linked to TB occur in places of poverty and marginalization in developed countries. According to the WHO (2016), population groups who are vulnerable to tuberculosis includes prisoners, injecting drug users, the homeless, ethnic minorities, and migrants – documented or undocumented, refugees, economic and labour migrants, asylum seekers – are those who experience access to health services is complicated by factors of social discrimination, poverty, and isolation.
Various political and socio-economic factors have recently surged the human migration rate, contributing to changes in different patterns of tuberculosis infection (Werf & Kramarz, 2016a). Many Western countries and Australia has seen an increase in TB infection with the influx of migrants and refugees (Rogo et al., 2017).
According to Tomas et al. (2013), in North America, Europe, and Australia, TB disproportionally impacts foreign-born populations that have migrated from Africa, Asia, and/or Latin America because TB infection rates in this area are much higher. In countries with low incidence, the infection rate among foreign-born migrants is ten to twenty times that of the autochthonous population (Tomás et al., 2013).
However, some studies indicate low infection rates in non-immigrant populations (Barniol et al., 2009). Still, the risk of transmission within the immigrant communities in the host country is very high.
Reactivation of latent TB infection is common among immigrant populations. It is considered the main reason behind many TB cases that occur even many years after the arrival of migrants into the host country. Current measures and interventions are not enough to detect latent TB and call for more active surveillance (Moore-Gillon, Davies, & Ormerod, 2010).
Notwithstanding the high proportion of TB cases among immigrants in low-incidence countries, there is an ensuing debate about the screening and educational programs and their public health impact. Research notes that TB control and treatment services in low-incidence countries that house a large population of immigrants face many challenges from the changing patterns of TB. The primary research question the current study looks to answer is;
How is latent tuberculosis tackled among immigrant populations in low-incidence Western countries and Australia regarding screening, educating, and adhering to patients’ treatments?
The current report looks to access and analyze relevant research literature to answer the research question. Understanding these factors plays an imperative role in evaluating and adapting the current programs and processes in place.
The general aim of this literature review is to explore screening processes for immigrants, their perceptions and knowledge of TB in addition to educational programs catered for them, and immigrant patient adherence to TB treatment. Using the developed research question and the study’s primary aim, the research objectives have been devised.
Three primary themes are being used to organize and analyze the literature review;
Many immigrant populations migrating to developed countries of the West and Australia are at higher risk of reactivating the latent TB disease. In many low-incidence industrialized countries with the high flux of immigration from less-developed countries, the general tuberculosis control strategies minimize transmission through identifying and curing a high portion of cases.
This strategy’s main components include early detection of TB, adequate treatment adherence for active infections, and detection and prophylactic treatment of latent infections, in some cases (Tomás et al., 2013). However, there is a notable difference between countries regarding screening and education programs for immigrants, such as screening/education locations, the programs’ administrative and financial costs, and legalities for providing care (Werf & Kramarz, 2016b; Wieland et al., 2012).
Often a migrant’s legal, economic and social circumstances can have detrimental impacts on the disease’s progression, diagnosis, treatment, and adherence to the scheme. Not only does this put immigrants at risk, but it also places a large risk to non-immigrant populations.
Immigrants face an array of issues in the process of migration which includes challenges like communication problems, adapting to new surroundings, loss of social support, acculturation, and discrimination which can be further aggravated by fear of TB, the stigmas associated with its diagnosis, fear of deportation, and changes that may need to be made when undergoing TB treatment.
Results from the current research can provide medical professionals insight into the macro-and micro-level impacts of TB on immigrant populations. Understanding these factors may lead to public health policy changes that are more lenient on immigrants and aid the wider community. Nurses can gain practical insight and knowledge from patient care results in immigrant populations with latent TB. The current study can also contribute to the existing literature to improve care and public health policies.
The current study uses a systematic literature review of qualitative, quantitative, and mixed methods studies. The literature review uses rigid methods and analysis to identify, evaluate and synthesize scientific evidence from primary studies on latent tuberculosis among immigrant populations.
According to Boland et al. (2013), a systematic literature review is designed to “locate, appraise, and synthesize” the best available evidence related to a specific research question to provide informed, evidence-based answers. In evidence-based nursing, a systematic literature review aids nurses in deciding whether the evidence is relevant to a particular patient.
It provides balanced clinical expertise pointing out the risks and benefits of specific procedures, treatments, and processes (Bettany-Saltikov, 2012). This study’s approach is relevant to tackling latent tuberculosis in immigrants allowing professionals insight into the screening process, adherence to treatment, views, and attitudes towards tuberculosis.
The current study’s Searches were carried out in the following databases: NCBI/PubMed, PLOS one, Embase, and Springer. These databases are used because of the number of articles they house and provide access to relevant topics to study.
Search topics in these databases included terms like “tuberculosis,” “immigrants,” “screening,” “adherence to treatment,” and “education” in combination with search terms and MeSH descriptions. The concept of “immigrant” in the current study uses a broad interpretation that includes asylum-seekers, economic refugees, and international migrants.
Refinement of search terms is essential to ensure that time is spent narrowing down appropriate literature (Holly, Salmond, & Saimbert, 2011). A second stage manual search was conducted on the selected articles’ bibliographies to identify the maximum possible relevant articles. A final internet search using Google Scholar was used to minimize the possibility of losing relevant sources.
| Database | Search Items | Results |
|---|---|---|
| NCBI/PubMed | #1 “tuberculosis” [Mesh] OR tb OR Tuberculosis. #2 “Migrants” [Mesh] OR “emigration and immigration” OR “refugees” [Mesh] OR immigrant* OR migrant OR refugee OR foreign. #3 “Screening” [Mesh] OR “prevalence” OR “testing” OR “prescreening” #4 “Education” [Mesh] OR “knowledge” OR “perceptions” #1 AND #2 AND #3 AND/OR #4. |
642 |
| PLOS One | #1 “tuberculosis” [Mesh] OR tb OR Tuberculosis. #2 “Migrants” [Mesh] OR “emigration and immigration” OR “refugees” [Mesh] OR immigrant* OR migrant OR refugee OR foreign. #3 “Screening” [Mesh] OR “prevalence” OR “testing” OR “prescreening” #4 “Education” [Mesh] OR “knowledge” OR “perceptions” #1 AND #2 AND #3 AND/OR #4. |
553 |
| Embase | #1 “tuberculosis” OR tb #2 “Migrants” OR “refugees” OR immigrant* foreign*. #3 “Screening” OR “prevalence” OR “testing” #4 “Education” OR “knowledge” OR “perceptions” #1 AND #2 AND #3 AND/OR #4 | 742 |
| Springer | Limits: Item type: Article; Data range from 2008 to 2017. #1 “tuberculosis” OR tb #2 “Migrants” OR “emigration and immigration” OR “refugees” OR refugee OR foreign. #3 “Screening” OR “testing” OR “pre-screening” #4 “Education” OR “knowledge” OR “perceptions” #1 AND #2 AND #3 AND/OR #4 |
1286 |
Both qualitative and quantitative studies were included in the systematic literature review. The search was limited to studies that were published in English. It was also necessary that publication remain recent, making it essential to limit the publication date from 2009-2017.
However, the study’s place was partially restricted in the search only to include industrialized Western countries and Australia. Studies that were literature reviews of any kind were excluded from the study.
Also, studies that had conducted any randomized control trial were excluded from this literature review. Such studies were excluded because they could not provide relevant data regarding the selected themes used to analyze the literature.
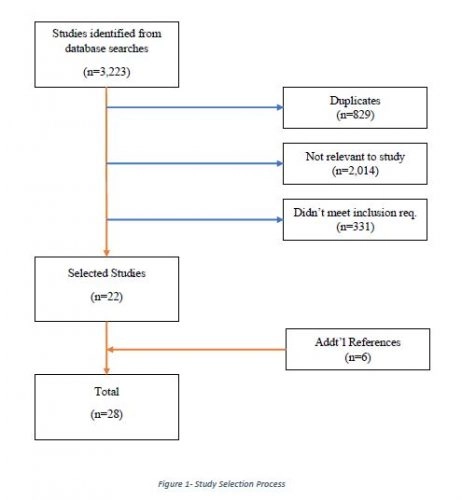
The initial results using the databased highlighted above identified a total of 3,223 articles. This was reduced to 2,394 articles when removing duplicates/overlapping articles from each database (829 duplicates). Afterward, titles and abstracts were reviewed, removing 2,041 articles since they were irrelevant to the research topic.
The 353 remaining articles were then read, both abstracts and full-text versions, resulting in 22 articles that were selected as meeting the inclusion criteria set above. Each of the articles’ bibliographies was then searched in addition to searches on Google Scholar, which further identified 6 articles that met the inclusion criteria. A total of 28 articles were finalized for inclusion in the literature review.
The selected articles were then compiled into a matrix to synthesize them based on the devised themes for analysis. The themes included are screening immigrants, education/knowledge of immigrants on latent tuberculosis, and adherence to immigrants’ treatments. The matrix of studies can be found in appendix A.
Baker (2014) asserted the necessity for becoming familiar with the work being analyzed to examine its relevance, strengths, and limitations to the research question when critiquing a piece of literature. Hence, the literature review uses the model developed by Caldwell et al. (2005) in critiquing literature (see fig.2) as the standard.
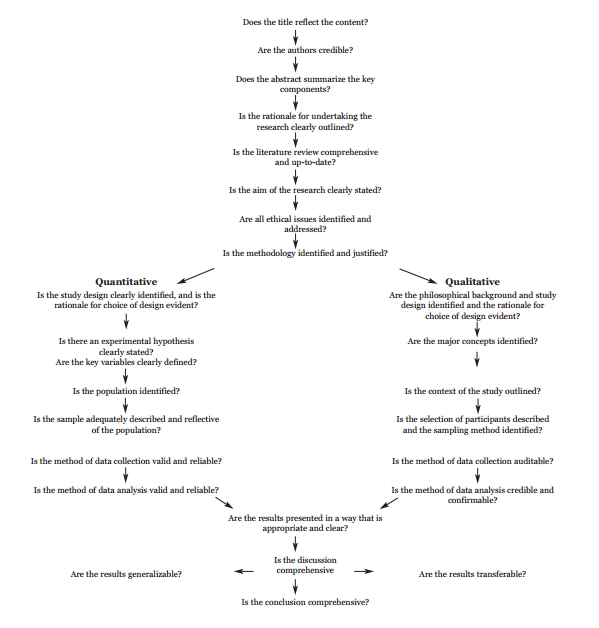
Figure 2- Research Critique Framework (Caldwell et al., 2005)
The model proposed by Caldwell et al. (2005) has a basic framework that breaks down the process of critiquing into four main questions that need to be answered.
This includes; ensuring that the literature review is current and comprehensive; if the sample is adequately described and reflective of the population for quantitative studies; if the selection criteria for recruiting patients is described and if a sampling method is identified for qualitative studies; and if the conclusion of the study is comprehensive (Caldwell et al., 2005).
A total of 28 articles were reviewed for the current literature review, with all the articles summaries and implications provided in Appendix A of this report. Complete analysis in this chapter of each piece of literature was not possible due to the current report’s word limit’s constrictions. Each of the articles presented one or more of the themes designated for analysis.
Each article is organized based on the themes they held and analyzed based on the Caldwell et al. (2005) model discussed earlier. The purpose of the investigation was to identify trends in the literature that may lead to contradictions or gaps/weaknesses that need to be filled.
Each piece of literature has been organized based on the themes being discussed and chronologically, based on the publication date from oldest to newest.
Panchal et al. (2013) study the potential impact on prospective TB incidence of implementing a strategy of targeted LTBI screening when immigrant registers with primary care. The study finds that LTBI screening at primary care registration provides an effective strategy for potentially identifying immigrants at high risk for developing TB (Panchal et al., 2013).
However, the study includes missing data into its statistical analysis, making it extremely probable for the study to have an extreme bias. The missing data is associated with the study’s cohorts’ attrition with internal migration away from the region during the observation period and the possibility of under ascertaining TB cases before 2006 (Panchal et al., 2013).
Schepisi et al. (2013) assessed adherence to and yield of TB screening programs based on symptom screening conducted at primary care centres for regular and irregular refugees/asylum seekers and immigrants in Rome, Italy. Evidence found that verbal symptom screening for TB of migrants in primary healthcare centres had yielded a higher percentage of migrants visiting specified TB clinics (Schepisi et al., 2013).
The study reports 254 individuals that provided at least one symptom of active TB during screening. Of these patients referred to a TB clinic, about half of them were present for further diagnosis and eventual treatment. A drawback to the study was the lack of detail on the screening model used.
The study does not outline TB symptoms used to determine a migrant’s eligibility to be recommended to TB clinics. It was found that 30 percent of migrants were not referred for further diagnostic evaluation (Schepisi et al., 2013), which ultimately questions the entire results.
Bennett et al. (2014) used TBHI screening results to analyze the prevalence of LTBI among the refugee population in San Diego, California, from January 2010 and October 2012. Based on the study, the screening initiative indicated 43 percent of cases with LTBI come from Sub-Saharan Africa (Bennett, Brodine, Waalen, Moser, & Rodwell, 2014).
The study found that these patients were less likely to initiate treatment than refugees from the Middle East. Bennett et al. (2014) also found that refugees with post-secondary education at minimum were more likely to participate in screening, understanding the disease, and then initiating treatment.
One of the study’s drawbacks is its methodology, which heavily relied on self-report data on factors such as smoking, diabetes, malignancy, ESRD, and education (Bennett et al., 2014). Therefore, there is an excellent chance of information bias which may have limited the variables’ accuracy or underreported because of perceived stigma.
Heuvelings et al. (2016) focus on screening techniques in European countries and Canada for LTBI. The study focuses the screening efforts placed on a category of the “vulnerable” population, including migrants, those of foreign birth, homeless people, drug/alcohol abusers, prisoners, and people with HIV in big cities (Heuvelings et al., 2016).
The study finds that screening uptake improves after vulnerable populations are specifically accommodated based on their unique needs (Heuvelings et al., 2016). The study is lacking in differentiating between populations and their correlations with screening. The study’s major research gap clans the screening effects into one broad category labelled “vulnerable population. Therefore, the study results are difficult to comprehend as generalizations are made to son in the study.
Pareek et al. (2016) examine the significance of LTBI on high-income countries with foreign-born patients to determine the best possible screening processes to lower the disproportionate burden of TB on these countries. The study focuses on multiple countries by reviewing their screening strategies in terms of yield and cost-effectiveness.
The study finds that common screening methods used for LTBI include tuberculin skin tests and interferon-gamma release assay, which is conducted post-arrival to the host countries (Pareek et al., 2016). The study finds that most high-income countries do not practice screening for LTBI. Do so post-arrival However, those who do, Pareek et al. (2016) see this method to be programmatically challenging to implement with the number of immigrants accepting and completing treatment to be suboptimal.
Zenner et al. (2017) examined the screening program Blackburn TST-based LTBI screening between 1989 and 2001 and further studied the treatment program between 2009 and 2013 that had used QuantiFERON (QFT) testing. According to the study, screening programs were aimed at recent migrants from high incidence TB areas identified through registrations with primary care physicians or a referral from the port of arrival (Zenner et al., 2017).
The comparative study of the two screening methods shows that there was a better predictive value of QFT than compared to TST. Zenner et al. (2017) also observe a greater reactivation rate of LTBI in the immigrant population, particularly immigrants from Southeast Asia, primarily from Pakistan and India.
However, there is a significant research gap found in Zenner et al.’s (2017) study, which is the length of the follow-up timing with participants being far-ranging and, in some cases, unknown. There are also cases in the study with participants that had entered the UK, resided, and then exited the UK (with the date of exit unknown), only to reenter again.
Tardin et al. (2009) aimed to analyze TB in a low-incidence area (i.e., area in Geneva) using a computerized database that had identified an unusually high proportion of patients coming from a specific country between 2004 and 2006. Aside from its primary aim, the study also conducted a cultural evaluation to examine the social stigma of TB in the community, especially for contact tracing methods.
The study was primarily quantitative, focusing on 13 patients diagnosed with TB and using RFLP (restriction fragment length polymorphism) analysis. Tardin et al. (2009) were able to identify all the possible ethical issues in the study. To maintain ethical credibility, Tardin et al. (2009) addressed these issues and maintained its integrity and participants.
The study’s main findings are the revelation that the community has the low acceptance of the diagnosis of TB as it’s considered a ‘dirty and sinful” disease that only impacts people of low status or living deprived life (Tardin et al., 2009). The study provided a cultural evaluation that allowed several strategies to use community characteristics to facilitate contact tracing by enhancing TB testing and portraying it as a desirable social behaviour.
Wieland et al. (2012) examine the use of English as a second language program at a community centre as the backdrop setting of understanding perceptions about TB among foreign-born persons. The study was qualitative in that it used focus groups as a means for data collection among 83 participants. The study found a plethora of misconceptions about the transmission of TB and nearly no knowledge of latent TB.
The hindrance to obtaining TB-related knowledge was practical consideration for the foreign-born participants, like transportation costs and conflicts with their work schedule.
Orders completed by our expert writers are
Butcher et al. (2013) examined 52 participants who were refugees and undergoing Isoniazid treatment for LTBI. The questionnaire distributed to participants focused on total knowledge and total side effects scores.
The study found a range of misconceptions about how TB was spread via water, dust, wind, or pollution (Butcher et al., 2013). These misconceptions impacted the patient’s willingness to take medication and comply with the treatment standards.
Colson et al. (2014) examine the TB knowledge, attitudes, and beliefs of foreign-born people in the US and Canada. The study finds that most participants had correctly answered their knowledge-based question son TB, while a majority also answered the perceived questions in the affirmative (Colson et al., 2014). Participants from Mexico and Latin America had a higher model adjusted knowledge score than immigrants from other world regions.
Gao et al. (2015) studied the knowledge and perceptions of LTBI among Chinese immigrants in Canada. The study is brilliantly executed by honing a specific immigrant population in a high-income low incidence country.
The study uses a mixed-methods methodology different from other studies discussed under this theme that used quantitative research approaches. Gao et al. first used a cross-section patient survey with focus group discussions with Chinese immigrants to understand the cultural perception of LTBI (2015).
The study results are significant as they suggest a significant concern in receiving the complex healthcare system. This took away the immigrant group’s want for testing and treatment.
Gao et al.’s (2017) focused on studying education material for immigrants regarding tuberculosis and LTBI. The study used a video that was a culturally tailored, multi-lingual, 4.5-minute health promotional video focused on LTBI with Canadian immigrants (Gao et al., 2017). Gao et al. (2017) found that 84 percent of viewers had found the video helpful while viewing the video caused a 21 percent increase in knowledge about LTBI.
This includes a significant increase in basic knowledge of LBTI transmission, symptoms, and treatments. However, the study did not focus on the video’s potential adverse effects, such as exaggerated fear, which can be considered an ethical ramification of conducting the study (Gao et al., 2017).
The study also lacked a long-term follow-up to determine if the knowledge that was gained was sustained. A major gap is the lack of clinical evidence that correlates knowledge acquisition to greater treatment or seeking screening.
Trauer and Krause’s (2011) study focused on newly arrived refugees from February 2006 to January 2009, studying the prevalence of latent TB and their adherence to treatments. The study found that older male patients from the Eastern Mediterranean region were associated with increased latent TB.
However, the results found that only 44 percent of refugees had completed treatment (Trauer & Krause, 2011). The common reason for discontinuation or non-adherence to treatments was gastrointestinal side effects and their loss to follow-up. There were no cultural obstacles to the acceptance of treatment or stigmas that hindered treatment regimes.
Nuzzo et al. (2013) looked to determine the proportion of refugee patients at the Baltimore City Health Department TB program completing their LTBI treatment compared to other referral groups. Examine 841 patients, and it was concluded that 81 percent of refugees had completed their LTBI treatments compared to 50 percent of non-refugee patients and 35 percent of US-born patients (Nuzzo et al., 2013).
The findings are not presented because the research approach mainly focused on quantitative research, which does not examine participant opinions or perspectives, keeping strictly to empirical analysis measures. This lack of analysis in the study prevents it from reaching its full potential and brings to question the conclusions drawn in the study.
The lack of explanation is a major research gap that needs to be filled to understand more refugees’ phenomena adhering to treatment than native-born patients.
Kan et al. (2013) aimed at studying treatment completion in refugees to identify factors associated with failure to complete preventive treatments. The study had found that younger patients from Somalia and asylum seekers were more likely not to complete their preventative treatments.
However, the trend of medication completers has increased by 16 percent, most like caused by a skewness from an influx of European immigrants (Kan et al., 2013). The skewed data used for comparison purposes in the study makes it more challenging to provide accurate conclusions to question the entire study.
Peluso et al. (2014) focused on analysing a student-run free clinic for LTBI patients in a predominately Hispanic immigrant community. The study found that their foundation, which focused on cultural case management, improved adherence to LTBI treatments. The free clinic model used matching patients and providers based on language competence and social or cultural affiliations (Peluso et al., 2014).
There was improved communication between patient and provider through shared language, direct phone call access, and patient-centred interviews (Peluso et al., 2014). The drawback to the study is that it used a relatively small sample size, making it difficult to draw definitive conclusions from the statistical comparison of factors linked to treatment outcome and adherence to treatment.
Subedi et al. (2015) examined the evaluation and treatment of LTBI in refugees at various member clinics of Philadelphia Refugee Health Collaborative (PRHC) vs. non-PRHC clinics. Subedi et al. (2015) examine a specific model implemented in PRHC practices hiring a bilingual refugee health service coordinator.
This resulted in refugees being screened in great proportion, attending follow-up appointments, and completing the course of treatment. The model studied bases its success on a multidisciplinary approach whereby doctors, nurses, social workers, and caseworkers manage refugees’ screening, evaluation, and treatment follow-up.
From the sample, 89 refugees completed follow-up appointments and 34 completed treatments in PRHC clinics compared to only 31 completing follow-ups and 9 completing treatments in non-PRHC clinics (Subedi et al., 2015).
Rogo et al. (2017), in their quantitative study, studied 120 patients with LTBI in Rhode Island. The study followed these participants over their 9-month course of Isoniazid, all of them being children. The study compared refugee patients with those who were not refugees to develop a basis for their conclusions.
The study has found a greater completion rate among refugee populations as they had adhered better to treatment regimes, especially among female patients. The refugee population also attended more scheduled visits compared to non-refugee patients in the study.
The literature review provides insight into the clinical issues related to screening, education, and adherence to treatment among immigrant populations with latent TB. Older studies in the current literature review, those pre-dating 2010, have shown that there is generally a low level of knowledge about latent TB and widespread misconceptions about the disease, especially regarding its transmission.
Some of the respondents in the studies did not have basic knowledge about the nature of bacteria and infection related to airborne transmission (Colson, Franks, Sondengam, Hirsch-Moverman, & El-Sadr, 2010; Nkulu, Hurtig, Ahlm, & Krantz, 2010; Wieland et al., 2012) but participants in other studies had attributed the disease to its correct facts (Colson et al., 2014; Gao et al., 2017; Rogo et al., 2017).
The attitudes and perceptions differed in each study based on its research location and the immigrant’s ethnicity group being studied. For example, in Gao et al. (2015), Chinese immigrants viewed the disease as irresponsible lifestyles or caused by living conditions, while the study conducted by Kan et al. (2013) found that Somali refugees considered TB to be a form of divine punishment for those that practiced a form of witchcraft or were dishonest.
When only focusing on immigrants’ education, the results provide insight into how the other three themes are impacted. With lack of education, more immigrants are likely not to adhere to preventive treatments, active treatments, and participate in screenings which were evident from the results obtained from studies like Bodenmann et al. (2009); Kulanes et al. (2010); Minodier et al. (2010); and Rogo et al. (2017).
Therefore, healthcare organizations and policy-making bodies need to widen their reach in immigrant populations to educate them on TB and latent TB. A greater awareness in the population will result in immigrants participating in a great deal more in screening and treatment. Heuvelings et al. (2016) found in their study that mobile screening units in Canada had increased the percentage of screenings in the country’s immigrant population.
Keeping in line with this service, it is recommended that low-incidence but high-income countries with large immigrant populations should invest in mobile health units dedicated to preventive diseases, like latent TB, to become available to their immigrant communities. A similar case was studied by Ospina et al. (2012), which found that community health workers improved screening and contact tracing among immigrants with TB in Barcelona.
Using a group of volunteer nurses, a mobile health unit’s strategy designated to specific areas that hold large populations of immigrants can help bring the incidence rate down. None of the literature reviewed in the current study has examined this particular strategy, most probably because it is non-existent.
However, this strategy’sactual implementation may be led to research in this area that focuses on mobile health units’ impact on screening, education, and adherence to treatment for latent TB.
The current study aimed to study how latent TB was tackled in the immigrant populations of low-incidence and high-income countries of the West and Australia. The literature review answered the research question to the fullest extent based on the available data. The current report uses 28 articles that were selected using the procedure of the systematic literature review.
Each of the articles was then analyzed using Caldwell et al. (2005) to critique academic literature. Based on the review, it is found that immigrant populations have a great lack of education in the topic of latent TB, often associated with their cultural misconceptions.
Articles published before 2010 found greater misinformation among immigrant populations, while more recent articles, particularly those published in 2017, saw a greater amount of awareness amongst them. The study has found various ways in which latent TB screening occurs, each differing based on the host country conducting the screening process.
However, most countries screen latent TB before the arrival of the host country. Studies have found that this allows for a greater chance of reactivation of latent TB among the immigrant population. There is no universal form of screening, causing disparities of TB incidences in each host country.
One of the most critical findings of the study was refugees’ great participation in adherence to TB and latent TB treatments compared to other forms of immigration and even native-born patients. Unfortunately, the studies analyzed could not provide the underlying cause for this phenomenon, proving a wide research gap in the literature.
Based on the literature review findings, a service improvement recommendation was made to improve the status of TB among immigrant populations in low-incidence, high-income countries.
The recommendation is made to healthcare organizations of such countries and policymakers – a greater effort in education and awareness programs targeted to immigrant communities in host countries. It was recommended that government and healthcare providers invest in mobile units dedicated to educating, screening, and providing treatment to immigrant communities for preventable diseases.
This recommendation’s justification comes from the literature review, which links a lack of education and knowledge to a lack of screening and non-adherence to treatments. This conclusion is based on correlation and not causation, as all the literature studied did not explain the relationship between these factors.
Barniol, J., Niemann, S., Louis, V. R., Brodhun, B., Dweck, C., Richter, E., … Junghanss, T. (2009). Transmission dynamics of pulmonary tuberculosis between autochthonous and immigrant sub-populations. BMC Infectious Diseases, 9, 197. https://doi.org/10.1186/1471-2334-9-197
Bender, A., Andrews, G., & Peter, E. (2010). Displacement and tuberculosis: recognition in nursing care. Health & Place, 16(6), 1069–1076. https://doi.org/10.1016/j.healthplace.2010.06.007
Bennett, R. J., Brodine, S., Waalen, J., Moser, K., & Rodwell, T. C. (2014). Prevalence and treatment of latent tuberculosis infection among newly arrived refugees in San Diego County, January 2010-October 2012. American Journal of Public Health, 104(4), e95–e102. https://doi.org/10.2105/AJPH.2013.301637
Bettany-Saltikov, J. (2012). How To Do A Systematic Literature Review In Nursing: A Step-By-Step Guide: A Step-By-Step Guide. McGraw-Hill Education (UK).
Bodenmann, P., Vaucher, P., Wolff, H., Favrat, B., de Tribolet, F., Masserey, E., & Zellweger, J.-P. (2009). Screening for latent tuberculosis infection among undocumented immigrants in Swiss healthcare centres; a descriptive exploratory study. BMC Infectious Diseases, 9, 34. https://doi.org/10.1186/1471-2334-9-34
Boland, A., Cherry, M. G., & Dickson, R. (2013). Doing a Systematic Review: A Student’s Guide. SAGE.
Butcher, K., Biggs, B.-A., Leder, K., Lemoh, C., O’Brien, D., & Marshall, C. (2013). Understanding of latent tuberculosis, its treatment, and treatment side effects in immigrant and refugee patients. BMC Research Notes, 6, 342. https://doi.org/10.1186/1756-0500-6-342
Colson, P. W., Couzens, G. L., Royce, R. A., Kline, T., Chavez-Lindell, T., Well, S., … Tuberculosis Epidemiologic Studies Consortium (TBESC). (2014). Examining the impact of patient characteristics and symptomatology on knowledge, attitudes, and beliefs among foreign-born tuberculosis cases in the US and Canada. Journal of Immigrant and Minority Health, 16(1), 125–135. https://doi.org/10.1007/s10903-013-9787-7
Colson, P. W., Franks, J., Sondengam, R., Hirsch-Moverman, Y., & El-Sadr, W. (2010). Tuberculosis knowledge, attitudes, and beliefs in foreign-born and US-born patients with latent tuberculosis infection. Journal of Immigrant and Minority Health, 12(6), 859–866. https://doi.org/10.1007/s10903-010-9338-4
Gao, J., Berry, N. S., Taylor, D., Venners, S. A., Cook, V. J., & Mayhew, M. (2015). Knowledge and Perceptions of Latent Tuberculosis Infection among Chinese Immigrants in a Canadian Urban Centre. International Journal of Family Medicine, 2015. https://doi.org/10.1155/2015/546042
Gao, J., Cook, V. J., & Mayhew, M. (2017). Preventing Tuberculosis in a Low Incidence Setting: Evaluation of a Multi-lingual, Online, Educational Video on Latent Tuberculosis. Journal of Immigrant and Minority Health, 1–10. https://doi.org/10.1007/s10903-017-0601-9
Guh, A., Sosa, L., Hadler, J. L., & Lobato, M. N. (2011). Missed opportunities to prevent tuberculosis in foreign-born persons, Connecticut, 2005-2008. The International Journal of Tuberculosis and Lung Disease: The Official Journal of the International Union Against Tuberculosis and Lung Disease, 15(8), 1044–1049. https://doi.org/10.5588/ijtld.10.0518
Holly, C., Salmond, S., & Saimbert, M. (2011). Comprehensive Systematic Review for Advanced Nursing Practice. Springer Publishing Company.
Kan, B., Kalin, M., & Bruchfeld, J. (2013). Completing treatment for latent tuberculosis: patient background matters. The International Journal of Tuberculosis and Lung Disease, 17(5), 597–602. https://doi.org/10.5588/ijtld.12.0692
Kulane, A., Ahlberg, B. M., & Berggren, I. (2010). “It is more than the issue of taking tablets”: the interplay between migration policies and TB control in Sweden. Health Policy (Amsterdam, Netherlands), 97(1), 26–31. https://doi.org/10.1016/j.healthpol.2010.02.014
Minodier, P., Lamarre, V., Carle, M.-E., Blais, D., Ovetchkine, P., & Tapiero, B. (2010). Evaluation of a school-based program for diagnosis and treatment of latent tuberculosis infection in immigrant children. Journal of Infection and Public Health, 3(2), 67–75. https://doi.org/10.1016/j.jiph.2010.02.001
Moore-Gillon, J., Davies, P. D. O., & Ormerod, L. P. (2010). Rethinking TB screening: politics, practicalities and the press. Thorax, 65(8), 663–665. https://doi.org/10.1136/thx.2009.132373
Nkulu, F. K., Hurtig, A.-K., Ahlm, C., & Krantz, I. (2010). Screening migrants for tuberculosis – a missed opportunity for improving knowledge and attitudes in high-risk groups: A cross-sectional study of Swedish-language students in Umeå, Sweden. BMC Public Health, 10(1), 349. https://doi.org/10.1186/1471-2458-10-349
Nuzzo, J. B., Golub, J. E., Chaulk, P., & Shah, M. (2013). Analysis of Latent Tuberculosis Infection Treatment Adherence Among Refugees and Other Patient Groups Referred to the Baltimore City Health Department TB Clinic, February 2009–March 2011. Journal of Immigrant and Minority Health, 17(1), 56–65. https://doi.org/10.1007/s10903-013-9882-9
Ospina, J. E., Orcau, À., Millet, J.-P., Sánchez, F., Casals, M., & Caylà, J. A. (2012). Community health workers improve contact tracing among immigrants with tuberculosis in Barcelona. BMC Public Health, 12(1), 158. https://doi.org/10.1186/1471-2458-12-158
Panchal, R. K., Browne, I., Monk, P., Woltmann, G., & Haldar, P. (2013). The effectiveness of primary care-based risk stratification for targeted latent tuberculosis infection screening in recent immigrants to the UK: a retrospective cohort study. Thorax, 69(4), 354–362. https://doi.org/10.1136/thoraxjnl-2013-203805
Pareek, M., Greenaway, C., Noori, T., Munoz, J., & Zenner, D. (2016). The impact of migration on tuberculosis epidemiology and control in high-income countries: a review. BMC Medicine, 14, 48. https://doi.org/10.1186/s12916-016-0595-5
Pareek, M., Watson, J. P., Ormerod, L. P., Kon, O. M., Woltmann, G., White, P. J., … Lalvani, A. (2011). Screening of immigrants in the UK for imported latent tuberculosis: a multicentre cohort study and cost-effectiveness analysis. The Lancet Infectious Diseases, 11(6), 435–444. https://doi.org/10.1016/S1473-3099(11)70069-X
Peluso, M. J., Hung, A., Lukasiewicz, A., Chang, H., Ramallo, J., Bartlett, M., … Ellis, P. (2014). Successful management of latent tuberculosis infection in an underserved community by a student-run free clinic. Journal of Health Care for the Poor and Underserved, 25(2), 837–862. https://doi.org/10.1353/hpu.2014.0109
Rogo, T., Eleanya, C., Hirway, P., Pelland, D., Lewis, C., Dennehy, P., & Losikoff, P. (2017). Adherence to Latent Tuberculosis Infection Treatment in a Population with a High Number of Refugee Children. Rhode Island Medical Journal (2013), 100(2), 34–38.
Schepisi, M. S., Gualano, G., Fellus, C., Bevilacqua, N., Vecchi, M., Piselli, P., … Girardi, E. (2013). Tuberculosis case finding based on symptom screening among immigrants, refugees, and asylum seekers in Rome. BMC Public Health, 13(1), 872. https://doi.org/10.1186/1471-2458-13-872
Subedi, P., Drezner, K. A., Dogbey, M. C., Newbern, E. C., Yun, K., Scott, K. C., … Johnson, C. C. (2015). Evaluation of latent tuberculous infection and treatment completion for refugees in Philadelphia, PA, 2010-2012. The International Journal of Tuberculosis and Lung Disease: The Official Journal of the International Union Against Tuberculosis and Lung Disease, 19(5), 565–569. https://doi.org/10.5588/ijtld.14.0729
Tardin, A., Dominicé Dao, M., Ninet, B., & Janssens, J.-P. (2009). Tuberculosis cluster in an immigrant community: case identification issues and a transcultural perspective. Tropical Medicine & International Health, 14(9), 995–1002. https://doi.org/10.1111/j.1365-3156.2009.02325.x
Tomás, B. A., Pell, C., Cavanillas, A. B., Solvas, J. G., Pool, R., & Roura, M. (2013). Tuberculosis in Migrant Populations. A Systematic Review of Qualitative Literature. PLOS ONE, 8(12), e82440. https://doi.org/10.1371/journal.pone.0082440
Torgerson, C. (2003). Systematic Reviews. A&C Black.
Trauer, J. M., & Krause, V. L. (2011). Assessment and management of latent tuberculosis infection in a refugee population in the Northern Territory. The Medical Journal of Australia, 194(11), 579–582.
Van der Werf, M. J., & Zellweger, J. P. (2016). Impact of migration on tuberculosis epidemiology and control in the EU/EEA. Euro Surveillance: Bulletin Europeen Sur Les Maladies Transmissibles = European Communicable Disease Bulletin, 21(12). https://doi.org/10.2807/1560-7917.ES.2016.21.12.30174
Werf, M. J. van der, & Kramarz, P. (2016). Tackling tuberculosis in migrants. The Lancet Infectious Diseases, 16(8), 877–878. https://doi.org/10.1016/S1473-3099(16)00148-1
Wieland, M. L., Weis, J. A., Yawn, B. P., Sullivan, S. M., Millington, K. L., Smith, C. M., … Sia, I. G. (2012). Perceptions of Tuberculosis Among Immigrants and Refugees at an Adult Education Center: A Community-Based Participatory Research Approach. Journal of Immigrant and Minority Health / Center for Minority Public Health, 14(1), 14–22. https://doi.org/10.1007/s10903-010-9391-z
Zenner, D., Loutet, M. G., Harris, R., Wilson, S., & Ormerod, L. P. (2017). Evaluating 17 years of latent tuberculosis infection screening in northwest England: a retrospective cohort study of reactivation. The European Respiratory Journal, 50(1). https://doi.org/10.1183/13993003.02505-2016
| Year; Name of Author(s) |
Full title of Article |
Title of Journal |
Country | Method | Findings | Implications |
|---|---|---|---|---|---|---|
| (2009) A. Tardin, M. Dominice Dao, B. Ninet3 and J.-P. Janssens | Tuberculosis cluster in an immigrant community: case identification issues and a transcultural perspective | Tropical Medicine and International Health | Geneva, Switzerland | Quantitative | Genotyping confirmed that 11 of 15 patients had identical isolates. Additional data revealed An unsuspected complex network of social links between 9 of these 11 patients. The transcultural evaluation pointed out the major obstacles to efficient contact tracing, such as the importance of social stigma related to TB, differences in communication style and health beliefs, and linguistic barriers. |
The combined finding of identical genotypes and important social links between patients confirmed a TB cluster’s suspicion due to recent transmission. The cultural evaluation helped explain the difficulties encountered during the contact tracing procedure and offered strategies to improve its efficacy despite the social stigma attached to TB in this community. |
| 2009) Patrick Bodenmann, Paul Vaucher1, Hans Wolff, Bernard Favrat, Fanny de Tribolet, Eric Masserey and Jean-Pierre Zellweger | Screening for latent tuberculosis infection among undocumented immigrants in Swiss healthcare centres; a descriptive exploratory study | BMC Infectious Diseases | Lausanne, Switzerland | Quantitative | Of the 161 participants, 131 (81.4%) agreed to screen, and 125 had complete examinations. Twenty-four of the 125 patients (19.2%; CI95% 12.7; 27.2) had positive interferon-assay results, two of which had active tuberculosis. Only five patients with LTBI completed full preventive treatments. Five others initiated the treatment but did not follow through. |
Screening for tuberculosis infection in this hard-to-reach population is feasible in dedicated urban clinics, and the prevalence of LTBI is high in this vulnerable population. However, low adherence to treatment is an important public health concerns and new strategies are needed to address this problem. |
| (2010) Faustine KK Nkulu, Anna-Karin Hurtig, Clas Ahlm and Ingela Krantz. | Screening migrants for tuberculosis – a missed opportunity for improving knowledge and attitudes in high-risk groups: A cross-sectional study of Swedish-language students in Umeå, Sweden | BMU Public Health | Umea, Sweden | Quantitative | Though most of them (72%) were screened, knowledge was poor with several misconceptions. The average knowledge score was 2.7 ± 1.3 (SD) (maximum = 8). Only 40 (15 %) of the 268 respondents answered at least half of the 51 knowledge items correctly. The average attitude score was 5.1 ± 3.3 (SD) (maximum = 12), meaning most respondents held negative attitudes towards TB and diseased persons. Up to 67% lacked knowledge about information sources, while 71% requested information in their vernacular. Knowledge level was positively associated with having more than 12 years of education and being informed about TB before moving to Sweden. The attitude was positively associated with years of education and having heard about the Swedish Communicable Disease Act but was negatively associated with being from the Middle East. Neither knowledge nor attitude was affected by health screening or exposure to TB information after immigration to Sweden. |
The majority had contact with Swedish health professionals through the screening process; knowledge about tuberculosis among these immigrants was low with several misconceptions and negative attitudes. Information may currently, be inaccessible to most immigrants due to the language barrier and unfamiliarity with the Swedish healthcare system. If TB education was included as a component of screening programs, ensuring that it was tailored to educational background, addressed misconceptions, and access problems could improve TB control in these communities. |
| (2010) Paul W. Colson, Julie Franks, Rita Sondengam, Yael Hirsch-Moverman, Wafaa El-Sadr | Tuberculosis Knowledge, Attitudes, and Beliefs in Foreign-born and US-born Patients with Latent Tuberculosis Infection | Journal of Immigration Minority Health. | Manhattan, NYC, USA | Quantitative | Of 251 participants, 66.5% were foreign-born. While misconceptions existed among US and foreign-born regarding transmission and contagiousness of LTBI, overall knowledge scores did not differ significantly between groups. Concerning attitudinal factors, foreign-born participants were less likely to acknowledge that they had LTBI and felt more ‘‘protected’’ from developing TB. |
Improved understanding of foreign-born patients’ KAB may reduce barriers to treatment and improve outcomes. People who immigrate to the United States increasingly represent the face of TB in the US. Effective measures to minimize barriers to LTBI treatment acceptance and completion depend on a better understanding of KAB among foreign-born patients who possess diverse views of LTBI and its treatment. |
| (2010) Kulanes, A., Ahlberg, B. M., and Berggren, I. | “It is more than the issue of taking tablets”: The interplay between migration policies and TB control in Sweden. | Health Policy | Stockholm, Sweden | Qualitative | Fear of being deported emerged as a barrier to sharing complete health information with the doctor. The routine contact tracing and follow-up of infected TB control cases were expressed as a source of concern since it was feared that healthcare providers could share the information with the immigration authorities. Interpreter use was expressed as a barrier, particularly if of the same female gender. |
It is important to know how a country’s immigration policies impact TB control activities among immigrants. The existing TB control measures, such as contact tracing, assume new meanings for immigrants. Further research is therefore needed to understand this emerging complexity to make TB control more effective. |
| (2010) Minodier, P., Lamarre, V., Carle, M. E., Blais, D.,Ovetchkine, P., and Tapiero, B. | Evaluation of a school-based program for diagnosing and treating latent tuberculosis infection in immigrant children. | Journal of Infection and Public Health. | Quebec, Canada | Quantitative | Four thousand three hundred and seventy-five children were offered screening, 82.3% consented to TST, and 22.8% were positive. Older age at migration (odds ratio (OR) = 1 [95% CI: 1.0—1.01]), as well as migration from a non-established market economy country (OR varying from 2.41 to 4.23), were significantly associated with positive TST. Further evaluation was refused in 5.7% among positive children, mainly in migrants from Eastern Europe (OR = 4.05 [95% CI: 2.14—7.69]). Refusal of treatment (11.2%) was more frequent in, Eastern European when compared to Southeastern Asian (OR = 6.91 [95% CI: 1.56—30.75]), in, blended families (OR = 3.25 [95% CI: 1.25—8.46]) and when the first hospital visit was delayed (OR = 1.01 [95% CI: 1.0—1.02]). Adequate completion of treatment was noted in 61.3%. Age > 16 years (OR = 1.82 [95% CI: 1.82—2.99]) |
A school-based TB screening program is effective if targeted towards recent immigrant children. Factors of refusal of testing and treatment seem essentially related to beliefs and behaviours concerning BCG vaccination protection, risks of LTBI, and TST ability to detect disease. Young age contributed to compliance. Improving treatment adherence requires a comprehension of socio-cultural beliefs and behaviours involved in LTBI and accessibility to TBClinics. |
| (2010) Bender, A., Andrews, G., Peter, E. | Displacement and tuberculosis: recognition in nursing care | Health & Place | Toronto, Canada | Qualitative | Awareness of displacement was expressed in nurses’ work in three particular ways: diminishing the social displacement of immigration, connecting here and there, and minimizing the displacement of contagiousness. These themes were evident in how nurses and clients got to know each other over the long course of treatment and came through aspects of clients’ homes as reflections of their identities and cultural learning exchanges related to past life experiences. Cultural learning exchanges refer to the learning that happened on both sides: nurses learning about other places in the world and clients learning about Canada, and how these exchanges contributed to shared understandings of the current place they were now in together. These themes were also there in the ways that nurses focused on and reacted to the condition. This involved paying attention to the individual issues of treatment, the fears and myths surrounding the disease, and concerns of infectiousness that also meant dealing with isolation. |
The study highlights the need to pay attention to displacement in building quality healthcare relationships. Furthermore, it calls attention to the importance, in TB practice specifically, of repeated clarifications about isolation and masking, and making conscious choices about proximity—where to sit or stand, how to greet, when to don masks and when to remove them, necessary to diminish feelings of fear and alienation. Likewise, it calls attention to the varied ‘support ’role in nursing. Public health professionals must critically question the value judgments made about places and the people living in them and advocate in meaningful ways that may serve to reinforce trust. Of course, the place cannot be considered sufficient in itself for understanding all relationships in nursing. Still, it certainly does lend a perspective on what nurses’ relational work means in certain contexts. |
| (2011) Trauer, J. M., and Krause, V. L. | Assessment and management of latent tuberculosis infection in a refugee population in the Northern Territory | The Medical Journal of Australia | Northern Territory, AUS | Mixed Methods | 458 of 465 eligible refugees were adequately assessed for LTBI, of whom 146 (31.9%) were diagnosed with LTBI. Older age, male sex, and World Health Organization Eastern Mediterranean region of birth were associated with increased prevalence of LTBI. Of the refugees diagnosed with LTBI, 10 failed to attend for follow-up, and 15 were not offered treatment. Isoniazid therapy was accepted by 93 of 121 refugees (76.9%), and 41 of these (44.1%) completed treatment. |
The most common reasons for discontinuation of therapy were medication-related side effects (most often gastrointestinal) and loss to follow-up. Increasing age was associated with failure to complete treatment. Outcomes of assessment and treatment for LTBI in newly arrived refugees in the NT are comparable to those for other target groups screened in developed countries. The loss to follow-up caused significant attrition in numbers, but complete data were obtained for a large proportion of eligible refugees. Most refugees who are offered treatment for LTBI accept, but less than half complete treatment. |
| (2011) Guh, A., Sosa, L., Hadler, J. L., and Lobato, M. N. | Missed opportunities to prevent tuberculosis in foreign-born persons, Connecticut, 2005-2008 | International Journal of Lung Diseases | Connecticut, USA | Qualitative | Of 161 foreign-born persons interviewed, 48% experienced TB disease within 5 years after arrival. One-third (51/156) reported having undergone post-arrival testing for LTBI. However, those with established health care providers were more likely to have reported testing (aOR 4.49, 95%CI 1.48–13.62); only 43% of such persons were tested. Undocumented persons, most of whom lacked a provider (53%), were less likely than documented persons to have reported testing (aOR 0.20, 95%CI 0.06–0.67). Hispanic permanent residents (immigrants and refugees) and visitors (persons admitted temporarily) were more likely than non- Hispanics in the respective groups to have reported testing (OR 5.25, 95%CI 1.51–18.31 and OR 7.08, 95%CI 1.30–38.44, respectively). |
The self-reported testing rate for LTBI among foreign-born persons in Connecticut with confirmed or suspected TB was low and differed significantly by ethnicity and immigration status. Strategies are needed to improve health care access for foreign-born persons and expanded testing for LTBI, especially among non-Hispanic and undocumented populations. |
| (2011) Pareek, M., Watson, J. P., Ormerod, L. P., Kon, O. M., Woltmann, G., White, P. J., Abu Bakar, I., Lalvani, A. | Screening of immigrants in the UK for imported latent tuberculosis: a multicenter cohort study and cost-effective analysis | Lancet Infectious Diseases | UK | Quantitative | Results for IGRA-based screening were positive in 245 of 1229 immigrants (20%), negative in 982 (80%), and indeterminate in two (0・2%). Positive results were independently associated with increases in tuberculosis incidence in immigrants’ countries of origin (p=0・0006), male sex (p=0・046), and age (p<0・0001). The national policy thus far would fail to detect 71% of individuals with latent infection. The two most cost-effective strategies were to screen individuals from countries with a tuberculosis incidence of more than 250 cases per 100 000 (incremental cost-effectiveness ratio [ICER] was £17 956 [£1=US$1・60] per prevented case of tuberculosis) and at more than 150 cases per 100 000 (including immigrants from the Indian subcontinent), which identified 92% of infected immigrants and prevented an additional 29 cases at an ICER of £20 819 per additional case averted. |
Screening for latent infection can be implemented cost-effectively at a level of incidence that identifies most immigrants with latent tuberculosis, thereby preventing substantial numbers of future cases of active tuberculosis. |
| (2012) Ospina, J. E., Orcau, A., Millet, J. P., Sanchez, F., Casals, and Cayla, J. A., | Community health workers improve contact tracing among immigrants with tuberculosis in Barcelona. | BMC Public Health | Barcelona, Spain | Quantitative | 960 foreign-born TB cases were detected, 388 in the intervention period. Contact tracing was performed on 65,7% of 201 smear-positive cases during the pre-intervention period compared to 81.6% of 152 smear-positive TB cases during the intervention period (p < 0.001). Risk factors associated with incomplete contact tracing of smear-positive index cases included being diagnosed in two hospitals without contact tracing TB unit (OR = 3.5; CI:1.4-8.9) and (OR = 4.6; CI:1.6-13.5) respectively, birth place in India-Pakistan (OR = 4.4; CI:1.9-10.3) or North Africa (OR = 4.3; CI: 1.8-10.5), having an unknown residence (OR = 5.4; CI:1.6-18.0), being HIV-infected (OR = 6.1; CI:2.5-14.8) or homeless (OR = 3.3; CI:1.3-8.2), and the absence of CHW intervention (OR = 2.4; CI:1.3-4.3). |
The effectiveness of contact tracing for TB control in high immigration areas can be improved by incorporating CHWs who act as translators, cultural mediators, and facilitators who accompany cases and contacts through treatment and follow-up. |
| (2012) Wieland, M. L., Weis, J. A., Yawn, B. P., Sullivan, S. M., Millington, K. L., Smith, C. M., Bertram, Ss., Nigon, J. A., and Sia, I. G. | Perceptions of tuberculosis among immigrants and refugees at an adult education centre: A community-based participatory research approach. | Journal of Immigration and Minority Health | Minnesota, USA | Qualitative | Multiple challenges with TB control and prevention were identified. There were various misperceptions about the transmission of TB and a lack of knowledge about latent TB. Feelings and perceptions related to TB included secrecy, shame, fear, and isolation. Barriers to TB testing include low awareness, lack of knowledge about latent TB, practical transportation, cost, and work schedule conflicts. Barriers to medication use include suspicion of generic medications and perceived side effects. |
Adult education centres with large immigrant and refugee populations as excellent venues for TB prevention and propose several recommendations for conducting these programs. Content should dispel the most compelling misperceptions about TB transmission while clarifying the difference between active and latent disease. Learners should be educated about TB in the US and that it is curable. Finally, TB programs that include learners and staff in their design and implementation provide greater opportunity for overcoming previously unrecognized barriers. |
| (2013) Nuzzo, J. B., Golub, J. E., Chaulk, P., and Shah, M. | Analysis of latent tuberculosis treatment adherence among refugees and other patient groups referred to the Baltimore City health department TB clinic, February 2009- March 2011 | Journal of Immigration and Minority Health | Maryland, USA | Quantitative | Among 841 patients evaluated by BCHD-TB and diagnosed with LTBI, 81 % of refugees, 50 % of non-refugee foreign-born, and 35 % of US-born patients completed LTBI treatment. In multivariate analysis, refugees had greater odds of LTBI treatment completion (Adjusted Odds Ratio 7.2; 95 % CI 4.2–12.4, p\0.001) compared to US-born individuals adjusting for age, gender, and treatment regimen. Overall, LTBI treatment completion remains suboptimal. At BCHDTB, LTBI treatment completion was significantly higher among refugees than other referral groups. Additional efforts are needed to optimize LTBI care, and future efforts may need to be tailored for different risk groups. |
Further research is urgently needed to determine the health system and patient factors associated with the lack of LTBI treatment completion among refugees. The significant observed differences in adherence to LTBI evaluation and treatment among refugees, non-refugee foreign-born, and US-born individuals suggests that TB programs may require different strategies to optimize LTBI care among different groups of patients. |
| (2013) Colson, P. W., Couzens, G. L., Royce, R. A., Kline, T., Chavez-Lindell, T., Welbel, S., Pang, J., Davidow, A., Hirsch-Moverman, Y. | Examining the impact of patient characteristics and symptomatology on knowledge, attributes, and beliefs among foreign-born tuberculosis cases in the US and Canada | Journal of Immigrant and Minority Health. | US & Canada | Quantitative | Of 1,475 participants interviewed, most answered the six knowledge items correctly. Significant predictors of correct knowledge included the region of origin, education, income, age, visa status, place of diagnosis, BCG vaccination, and TB symptoms. Significant predictors of higher perceived risk/stigma scores included the region of origin, age, place of diagnosis, English fluency, time in the US/Canada, TB symptoms, and household rooms. This study examines associations between TB KAB and patient and disease characteristics in foreign-born individuals in the US/Canada. |
This study is the first attempt to uncover associations between TB KAB and patient and disease characteristics. Many participants could not answer knowledge items that suggest a role for improved health education for the foreign-born. The findings call for improved health education and efforts to reduce stigma and enhance realistic risk assessments. |
| (2013) Kan, B., Kalin, M., and Bruchfeld, J. | Completing treatment for latent tuberculosis: Patient background matters | International Journal of Tuberculosis and Lung Disease | Stockholm, Sweden | Quantitative | Younger patients, patients originating from Somalia, and asylum seekers were more likely to be non-completers. The proportion of completers increased from 71% in 2002 to 87% in 2007. However, this trend appears to be caused mostly by an increase in the proportion of European patients. |
The finding of a low rate of treatment completion among Somalis should be regarded as a call for intervention on the individual patient level, taking into account socio-cultural aspects such as perceptions of health care by the Somali community. Treatment completion continues to be of concern as it is not improving among risk populations. |
| (2013) Schepisi, M. S., Gualano, G., Fellus, C., Bevilacqua, N., Vecchi, M., Piselli, P., Battagin, G., Silvestrini, G., Attanasio, A., Vela, A., Rocca, G., Rinaldi, A., Benedetti, P., Geraci, S., Lauria, F. N., and Girardi, E. |
Tuberculosis case finding based on symptom among immigrants, refugees, and asylum seekers in Rome. | BMC Public Health | Rome, Italy | Quantitative | Among 2142 migrants enrolled, 254 (11.9%) reported at least one symptom suggestive of active tuberculosis, and 176 were referred to the tuberculosis clinic. Of them, 80 (45.4%) did not present for diagnostic evaluation. Tuberculosis was diagnosed in 7 individuals representing 0.33% of those screened and 7.3% of those evaluated for tuberculosis. |
This intervention’s overall yield was in the range reported for other tuberculosis screening programs for migrants, although we recorded an unsatisfactory adherence to diagnostic workup. Possible advantages of this intervention include low cost and reduced burden of medical procedures for the screened population. Further evaluation of this approach appears to be warranted. |
| (2013) Panchal, R. K., Browne, I., Monk, P., Woltmann, G., Haldar, P. | The effectiveness of primary care-based risk stratification for targeted latent tuberculosis infection screening in recent immigrants to the UK: A retrospective cohort study. | Thorax | UK | Quantitative | 250 cases (29%) were potentially preventable in Flag-4-registered immigrants. Overall, 511 cases (60%) were potentially preventable among primary-care registered immigrants, implying a significant proportion without Flag-4 status. Prospective TB incidence (95% CI) after Flag-4 registration was 183 (163 to 205) cases/ 100 000 person-years, with a NNS (95% CI) of 145 (130 to 162). Targeted screening was most effective for 16–35 year olds from TB incidence regions 150–499/ 100 000 (NNS (95% CI)=65 (57 to 74), preventing 159 (18.7%) cases). Unpreventable TB risk increased with delayed primary care registration after UK entry (p<0.001) and was associated with HIV seropositivity (relative risk (95% CI) =1.89 (1.25 to 2.84), p=0.003). |
LTBI screening at primary care registration offers an effective strategy for potentially identifying immigrants at high risk of developing TB. |
| (2013) Butcher, K., Biggs, B. A., Leder, K., Lemon, C., O’Brien, D., Marshall, C. | Understanding of latent tuberculosis, its treatment, and treatment side effects in immigrant and refugee patients. | BMC Research Notes | Victoria, AUS | Quantitative | Fifty-two participants were recruited, 20 at isoniazid commencement and 32 already on isoniazid. The average TKS were 5.04/9 and 6.23/9, respectively, and were significantly associated with interpreter use. Approximately half did not know how tuberculosis was transmitted. The average TSES were 5.0/7 and 3.5/7, respectively, but were not influenced by socio-demographic factors. |
There was suboptimal knowledge about LTBI. Improvements in health messages delivered via interpreters and additional distributing information methods need to be developed for this patient population. |
| (2014) Bennett, R. J., Brodine, S., Waalen, J., Moser, K., Rodwell, T. C. | Prevalence and treatment of latent tuberculosis infection among newly arrived refugees in San Diego Country, January 2010- October 2012 | American Journal of Public Health | California, USA | Quantitative | The prevalence of LTBI was highest among refugees from sub- Saharan Africa (43%) and was associated with current smoking and having clinical comorbidity that increases the risk for active tuberculosis. Although refugees from sub-Saharan Africa had the highest prevalence of infection, they were significantly less likely to initiate treatment than refugees from the Middle East. Refugees with postsecondary education were significantly more likely to initiate LTBI treatment. |
Public health strategies are needed to increase treatment rates among high-risk refugees with LTBI. Particular attention is required among refugees from sub-Saharan Africa and those with less education. |
| (2014) Peluso, M. J., Hung, A., Lukasiewicz, A., Chang, H., and Ramallo, J. | Successful management of latent tuberculosis infection in an underserved community by a student-run free clinic | Journal of Health Care for the Poor and Underserved | Connecticut, USA | Quantitative | The number of TSTs placed in our clinic varies each year; for example, in 2011, there were 49 TSTs placed, of which 19 (40%) were positive, and 15 patients were treated, while in 2012, there were 28 TSTs placed and only four were positive and treated. Patient-reported medication adherence, recorded in self-reported pills taken per month, was high (29/ 30 pills/ month) and did not differ between the treatment outcome groups. When asked about barriers to taking their medication, patients most commonly cited forgetting to take the INH (n = 16; 41%) or denied any specific barriers (n = 16; 41%). Other barriers included side effects (n = 6), desire to drink alcohol (n = 2), and household duties (n = 1). Liver function tests were ordered at least once during treatment in 16/ 39 (41.2%) patients in the program. |
Cultural case management, or matching patients and providers based on language competence and social or cultural affiliation, may improve adherence. Improved communication through shared language, direct phone access, and a patient-centred interview model may have contributed to patient adherence and satisfaction with the program. The patient-provider relationship was also enhanced by the number of program encounters permitted by our high provider-patient ratio and the accessibility of our providers. Finally, the TB Advocates provided counselling focused on outreach, adherence, and refill reminders, which others have shown to improve adherence. |
| (2015) Subedi, P., Drezner, K. A., Dogbey, M. C., Newbern, E. C., Yun, K., Scott, K. C., Garland, J. M., Altshuler, M. J., and Johnson, C. C. | Evaluation of latent tuberculosis infection and treatment completion for refugees in Philadelphia, PA, 2010-2012 | International Journal of Tuberculosis and Lung Disease | Pennsylvania, USA | Quantitative | Of the 2094 refugees who arrived in Philadelphia in 2010–2012, the Philadelphia Department of Public Health notified 149 who required additional TB evaluation. Among these, 57 (38.3%) were confirmed to have LTBI, and none were diagnosed with active TB. All LTBI cases were recommended for anti-tuberculosis prophylaxis, and 43 (75.4%) completed treatment. Refugees receiving care from PRHC clinics were more likely to be screened within 30 days of arrival (OR 4.70, 95%CI 2.12–10.44), attend a follow-up appointment (OR 4.53, 95%CI 1.36–16.27), and complete treatment (OR 9.44, 95%CI 2.39–37.3) |
Refugees who attended PRHC clinics were more likely to be evaluated promptly and complete LTBI treatment. The PRHC clinics serve as a model for communities seeking to improve refugee health care. |
| (2015) Gao, J., Berry, N. S., Taylor, D., Venners, S. A., Cook, V. J., Mayhew, M. | Knowledge and perceptions of latent tuberculosis infection among Chinese immigrants in Canadian urban centre. | International Journal of Family Medicine | Canada | Mixed Methods | The survey identified a mean basic knowledge score: 40.0% (95% CI: 38.3%, 41.7%). FGDs confirmed that Chinese immigrants’ knowledge of LTBI was low, and they confused it with TB disease to the extent of experiencing LTBI associated stigma. Participants also expressed difficulties navigating the health system, which impeded testing and treatment of LTBI. Online videos were the preferred format for receiving health information. |
Identified striking gaps in knowledge surrounding an LTBI diagnosis. Concerns of stigma may influence acceptance and adherence to LTBI treatment in Chinese immigrants. Integrating these findings into routine health care is recommended. |
| (2016) Heuvelings, C. C., de Vries, S. G., and Grobusch, M. P. | Tackling TB in low-incidence countries: Improving diagnosis and management in vulnerable populations. | International Journal of Infectious Diseases | Canada & Europe | Qualitative | In low tuberculosis incidence regions, tuberculosis is mainly concentrated among hard-to-reach populations like migrants, homeless people, drug or alcohol abusers, prisoners, and people living with HIV. To eliminate tuberculosis from these low-incidence regions, tuberculosis screening, and treatment programs should focus on these hard-to-reach populations. |
Screening by chest X-ray (CXR) is an effective and cost-effective intervention among all vulnerable populations. Adding sputum culture to CXR screening as a pre-migration screening tool for migrants from high-incidence countries increase the number of TB diagnoses in the home country. It reduces the importation of TB into the host country. As spearheaded by non-affluent countries with a high burden of co-infections, collaborative TB/HIV prevention and treatment frameworks need to be further developed to reduce the burden of TB in people living with HIV to reduce the burden of HIV people diagnosed with TB. |
| (2016) Pareek, M., Greenway, C., Noori, T., Munoz, J., and Zenner, D. | The impact of migration on tuberculosis epidemiology and control in high-income countries: A review | BMC Medicine | Multiple | Qualitative | Migrants with LTBI are coming to lower incidence settings. In the initial years following arrival in the destination country, have a higher risk of LTBI reactivation which decreases slowly over time but remains higher than rates in the host population. This higher rate of reactivation in the initial one to two years after migrants arrive likely reflects latent tuberculosis infection acquired in their country of origin shortly before migration. However, there is also an ongoing complex interplay, in the destination country, of host and environmental factors that contribute to the observed epidemiology. |
The burden of disease in the foreign-born migrant population is primarily due to high TB burden settings migration and the reactivation of remotely-acquired latent TB infection. Consequently, there is an increasing focus on how best to enhance TB control through the coordinated screening of migrants for TB. Most countries focus on screening migrants for active TB, and this has a relatively low yield on its own and, likely, the most effective and cost-effective means of screening migrants for TB will comprise multiple, inter-linking elements: pre-arrival screening for active TB and targeted post-arrival screening for LTBI in migrants from intermediate/high TB burden settings. |
| (2017) Zenner, D., Loutet, M. G., Harris, R., Wilson, S., and Ormerod, L P. | Evaluating 17 years of latent tuberculosis infection screening in north-west England: A retrospective cohort study of reactivation. | European Respiratory Journal | England, UK | Quantitative | 97 out of 1820 individuals screened for LTBI were reported to have active TB. Crude incidence rates among LTBI-positive, treatment-naïve individuals were 4.1 and 2.3 per 100 person-years in the QuantiFERON and tuberculin skin test cohorts, respectively. Among the QuantiFERON cohort, Poisson regression showed that LTBI positivity (IRR 22.6, 95% CI 6.8–74.6) and no chemoprophylaxis increased the probability of becoming a TB case (IRR 0.17, 95% CI 0.05–0.6). |
High TB rates in LTBI-positive, treatment-naïve individuals and a strong association between no treatment and becoming a TB case, demonstrating feasibility and effectiveness of LTBI screening and providing important policy lessons for LTBI screening in England and beyond. |
| (2017) Gao, J., Cook, V. J., and Mayhew, M. | Preventing tuberculosis in low incidence setting: Evaluation of Multi-lingual, online, educational video on latent tuberculosis | Journal of Immigrant and Minority Health | Canada | Mixed Methods | Of 1598 survey respondents, 193 viewers had a mean knowledge score of 59%, compared to 38% in non-viewers. Eighty-four percent of viewers rated the video as helpful. When controlling for other factors, viewing the video was associated with a 1.04 (95% CI 0.85–1.26) or a 21% increase in a knowledge score. Qualitative data suggested the video was acceptable and may facilitate behaviour change. This online educational video shows promise as a tool to supplement clinical care. |
Viewing the video alone was associated with a modest but statistically significant increase in basic knowledge about LTBI transmission, symptoms, and treatment. Given the basic knowledge evaluated in the survey, it was reasonable to expect that viewing the video alone could result in a near-perfect score. Yet, it was only associated with a mean knowledge score of 59%, 21% higher than non-viewers. This finding illustrates the importance of reinforcing messages through other means |
| (2017) Rogo, T., Eleanya, C., Hirway, P., Pelland, D., Lewis, C., Dennephy, P., and Losikoff, P., | Adherence to latent tuberculosis infection treatment in a population with many refugee children. | Rhode Island Medical Journal | Rhode Island, USA | Quantitative | Of 120 patients with LTBI, 93% were foreign-born, and 30% were refugees. Overall, 94 children (78.3%) completed therapy. Higher treatment completion rates were seen among female patients referred within the same hospital the system, using an interpreter and did not report side effects. Refugees attended more scheduled visits compared to non-refugees (p=0.019). |
Overall rates of completion of LTBI treatment were high in this population. Better adherence to clinic visits, likely due to the increased support and care coordination provided to the refugee children, improved treatment completion rates. |
To write a master’s level literature review:
All work is written by human writers. 100% AI free, guaranteed.

100% money back guarantee if you find plagiarism in our work.
COMPANY DETAILS